If you've ever researched testosterone, whether out of curiosity, concern, or desperation, you've probably encountered dozens of products claiming to "boost" it. Testosterone boosters, optimizers, maximizers, amplifiers. The labels are creative. What they almost never tell you is where in the production chain they claim to act, or whether they act on the production chain at all.
To evaluate any of those claims, you need to understand the system your body uses to produce testosterone. It's called the hypothalamic-pituitary-gonadal axis, the HPG axis for short. Most men have never heard of it. But once you understand it, you'll never look at a testosterone product the same way again.
The Chain: From Brain to Bloodstream
Testosterone production isn't a single event. It's a cascade, a chain of chemical signals that starts in your brain and ends in your testes. Each link in the chain depends on the one before it. If any link breaks or weakens, the entire chain underperforms.
Here's how it works, step by step.
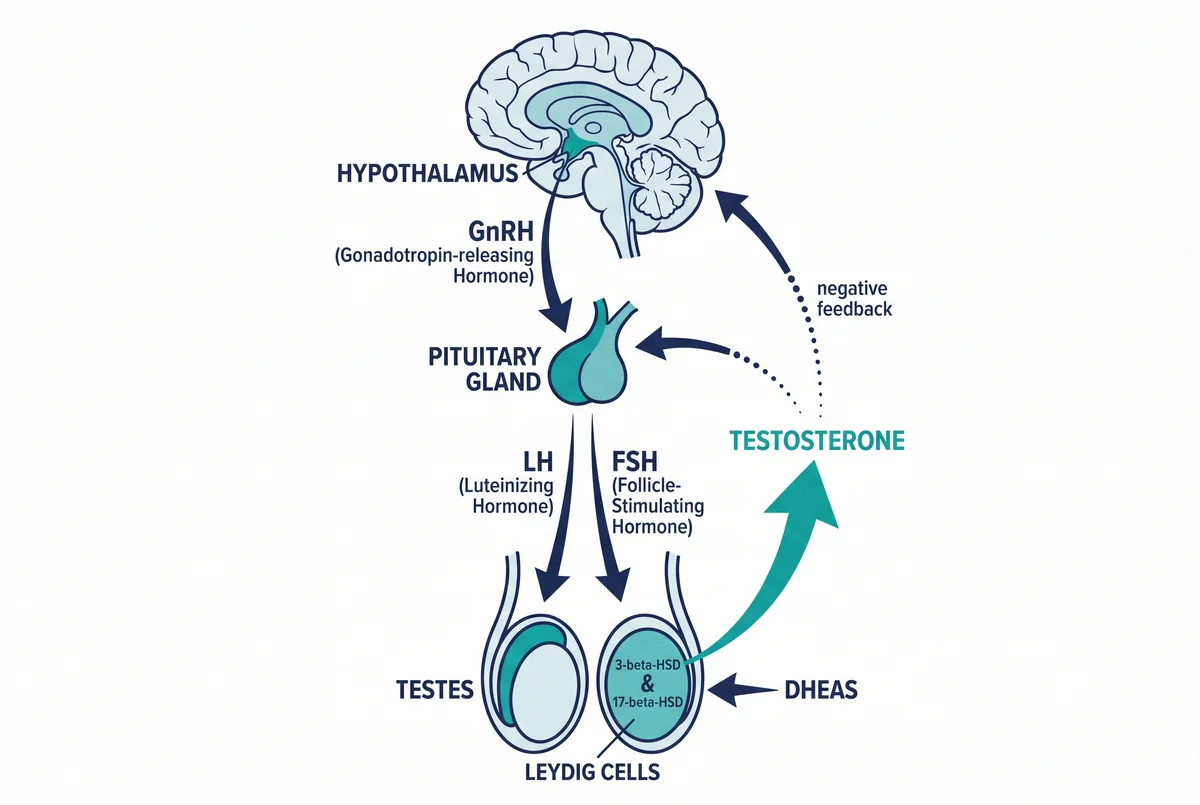
The HPG Axis, Testosterone Production Chain
This cascade is elegant in its simplicity. Brain senses low T, sends a signal, testes respond, testosterone rises, brain dials down the signal. A self-regulating loop that, when functioning properly, maintains hormonal balance without any external input.
What Happens When Each Link Breaks
Understanding the chain means understanding the specific ways it can fail. Each failure point produces a different clinical picture and demands a different solution.
Hypothalamic Dysfunction
The hypothalamus is exquisitely sensitive to stress, sleep deprivation, caloric restriction, and environmental disruption. Chronic stress elevates cortisol, which directly suppresses GnRH pulsatility. If the hypothalamus doesn't send the signal, the entire downstream chain goes quiet, even if the pituitary and testes are perfectly healthy.
This is why severe dieting, overtraining, and chronic sleep deprivation can tank testosterone. The machinery is intact. The starting signal just isn't firing.
Pituitary Issues
The pituitary can be suppressed by certain medications (opioids are notorious for this), head trauma, or tumors. If the pituitary doesn't produce adequate LH in response to GnRH, the testes never get the memo. Bloodwork in this case shows low LH alongside low testosterone, a pattern called secondary hypogonadism.
Leydig Cell Damage or Dysfunction
The Leydig cells themselves can be damaged by environmental toxins, varicocele, infections like mumps orchitis, or simply age-related attrition. When Leydig cells lose function, the brain sends more and more LH trying to stimulate production, but the testes can't respond. Bloodwork shows high LH alongside low testosterone, primary hypogonadism.
The distinction between primary and secondary hypogonadism is clinically critical but rarely discussed outside endocrinology. It determines not just the diagnosis but the appropriate intervention. And it's the lens through which every testosterone product should be evaluated.
The Critical Question: Support vs. Replace
Once you understand the HPG axis, a fundamental question emerges about any testosterone intervention: does it support the chain, or does it bypass it?
This distinction is everything.
Why TRT Bypasses the Chain
Testosterone Replacement Therapy, injecting exogenous testosterone, delivers the end product directly into the bloodstream. Testosterone levels rise immediately. You feel better. Problem solved, right?
Not exactly. Remember the feedback loop. When the hypothalamus detects high circulating testosterone, it shuts down GnRH production. No GnRH means no LH. No LH means the Leydig cells receive no stimulation. They atrophy. The testes literally shrink because they're no longer being asked to do their job.
This is why TRT creates dependency. It doesn't fix why your body stopped making testosterone. It replaces your body's function entirely. Stop the injections and you're left with a suppressed HPG axis and atrophied Leydig cells, often with lower natural production than you started with. For some men with genuine primary hypogonadism, TRT may be the only viable option. But for the much larger population of men with functional, lifestyle-driven, or age-related decline, it's a sledgehammer where a scalpel might suffice.
Why Most Supplements Don't Reach the Chain
On the other end of the spectrum, most over-the-counter testosterone boosters don't interact with the HPG axis in any meaningful way. They work peripherally, if they work at all. Some claim to inhibit aromatase (reducing testosterone-to-estrogen conversion). Some claim to lower SHBG (freeing up bound testosterone). Some are simply multivitamins with a testosterone label slapped on.
None of these approaches address the core production chain. They're rearranging deck chairs on the Titanic. If your body isn't producing enough testosterone because the HPG axis is underperforming, no amount of aromatase inhibition or SHBG modulation will fix the root problem. You need something that supports the chain itself, from hypothalamic signaling through Leydig cell function.
What Real HPG Axis Support Actually Looks Like
This is the question I spent years trying to answer. If you wanted to design a natural protocol that genuinely supports testosterone production, what would it need to do?
The honest answer, and the one that took me longest to accept, is that it would need to operate at multiple links of the chain at the same time. No single compound has clinical evidence of supporting every step of the HPG axis on its own.
A protocol that actually works has to cover, at minimum:
- Brain-level signaling. Maintain GnRH and LH release. Don't suppress them.
- Stress regulation. Lower chronic cortisol, which directly suppresses GnRH and pulls pregnenolone away from testosterone synthesis.
- Leydig cell support. Keep the cells that actually produce testosterone healthy and responsive to LH.
- Enzymatic cofactors. Provide what 3β-HSD, 17β-HSD, and the other enzymes in the conversion pathway need to work.
- Free testosterone availability. Reduce SHBG binding so the testosterone you produce is actually bioavailable.
- Feedback loop preservation. Support the chain, never replace it from outside.
- Real, standardized active compounds at clinically meaningful doses. Most "supplements" fail here before they ever fail mechanistically.
That's a multi-pressure-point intervention. Not a miracle ingredient. And it's the framework that finally moved my own bloodwork from 187 to 566 ng/dL after years of single-ingredient experiments that went nowhere.
The compounds that hit each pressure point exist. The clinical evidence is published. What's much rarer is finding them assembled into one protocol, with the active compounds genuinely standardized, and with the real doses actually present in the bottle. I cover each individual compound and its evidence in separate articles on this site, and my personal account of how I built the protocol I now take is in my main piece.
Why This Framework Matters
The HPG axis isn't just an academic concept. It's a practical evaluation tool.
The next time you see a testosterone product, ask one question:
Where does this act on the chain, and does it cover every link?
If the answer is "it delivers exogenous testosterone," you know it will suppress the feedback loop and create dependency.
If the answer is "it works peripherally" or "it only acts on one node," it can't move the full system. The chain is only as strong as its weakest link, and supporting one link while ignoring the others is exactly why most testosterone supplements fail to move bloodwork in any meaningful way.
If the answer is "we don't know," which is the honest answer for most products, then you're taking something on faith, not on evidence.
And if the answer is "it supports every link in the chain with a separate, standardized, clinically backed compound, and the data confirms elevated total testosterone alongside maintained LH and FSH," then you've found something worth investigating further.
That's the bar. It's a high one. Most products fail it. The few that pass are the only ones worth taking seriously.
This article is part of a series on male hormonal science. For the evidence framework I use to evaluate supplement studies, see my article on why most supplement studies are worthless. For deep dives into individual compounds that act on specific HPG pressure points, see my reviews of Shilajit's clinical data (testes, enzymatic conversion) and Tongkat Ali and Ashwagandha (Leydig support and cortisol modulation).